


业务咨询

![]() 发布时间:2023-05-26
发布时间:2023-05-26
![]() 环特生物
环特生物
![]() 浏览次数:6187
浏览次数:6187
原文献:Lee, H.S., Han, D.H., Cho, K. et al. Integrative analysis of multiple genomic data from intrahepatic cholangiocarcinoma organoids enables tumor subtyping. Nat Commun 14, 237 (2023).
编者按:肝内胆管癌(Intrahepatic Cholangiocarcinoma,ICC)是一种预后极差的肿瘤疾病,其5年生存率低于20%,大多数患者在诊断时已到达晚期[2, 3]。在第5版世界卫生组织肿瘤分类中ICC被分为大导管(LD)和小导管(SD)两种亚型 [6-14]。尽管预计这两种类型肿瘤的起源、癌变以及对化疗的反应会存在差异,但由于缺乏合适的体外模型,难以获得足够的肿瘤组织等原因,对这些差异的深入研究存在一定的困难。
近期有研究成功从胆管癌样本中培养出成人体干细胞衍生的肿瘤类器官[15-20],其显示出与原发性肿瘤相似的表型与遗传特征。基于此,研究人员使用患者来源的类器官进行组织学亚型的前瞻性建模。结合基因组分析技术,进一步确定了ICC患者潜在的特定类型靶向通路,以便有利于未来的个性化治疗。
一、研究结果
1. ICC类器官具有患者原发肿瘤的特征
HE染色结果显示来源ICC肿瘤患者的类器官拥有与原发性肿瘤相似的表型,免疫荧光结果显示其特异性表达胆管细胞标记物KRT19和SOX9,而未见肝细胞标记物AFP和白蛋白。进一步对ICC类器官中PD-L1的表达进行分析,发现其与原发性肿瘤组织中PD-L1的表达水平相匹配。
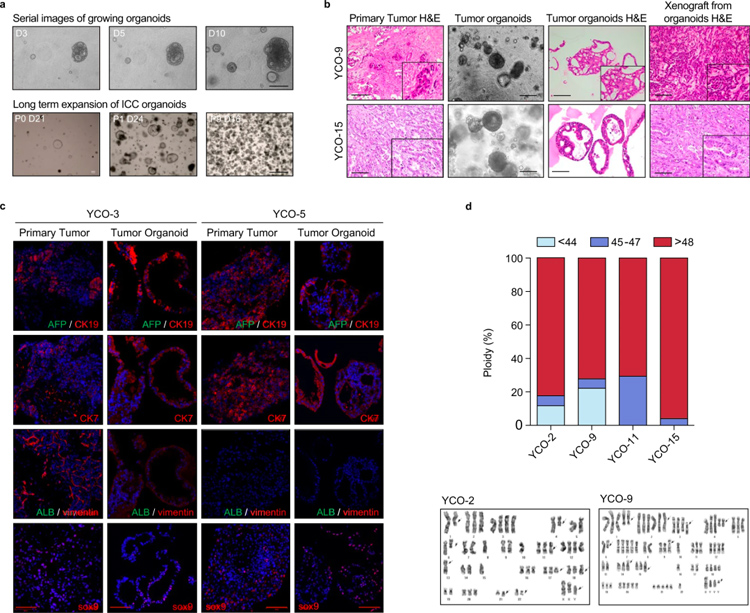
图1
2、ICC类器官能够对胆管癌肿瘤亚型进行分类
最近的研究表明,根据S100P、N-cadherin和CD56的表达,ICC可分为LD型(S100P+)和SD型(N-cadherin+CD56+)。原发性肿瘤与相应类器官的组织学分析显示,肿瘤与类器官中都含有紧凑、小而圆形的细胞。免疫组化的结果证实了预期的亚型分类,即LD型(S100P+)和SD型(N-cadherin+CD56+)。该分析结果表明肿瘤组织样本和类器官样本相互匹配。
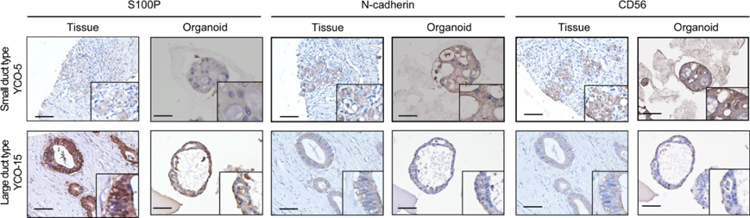
图2
对原始肿瘤组织和类器官之间的遗传相似性进行评估,28个样本中(13个原始肿瘤和15个肿瘤类器官)有27个(96.4%)表现出体细胞突变,包括TP53、BAP1、KRAS、ARID1A和IDH1/2的突变。与LD型相比,SD型样本具有高比例的BAP37和IDH2/12突变,而SBS1在LD型样本中更频繁地表达。上述数据表明体细胞突变可同时存在于在原发肿瘤标本和类器官之中,其一致性高于70%。
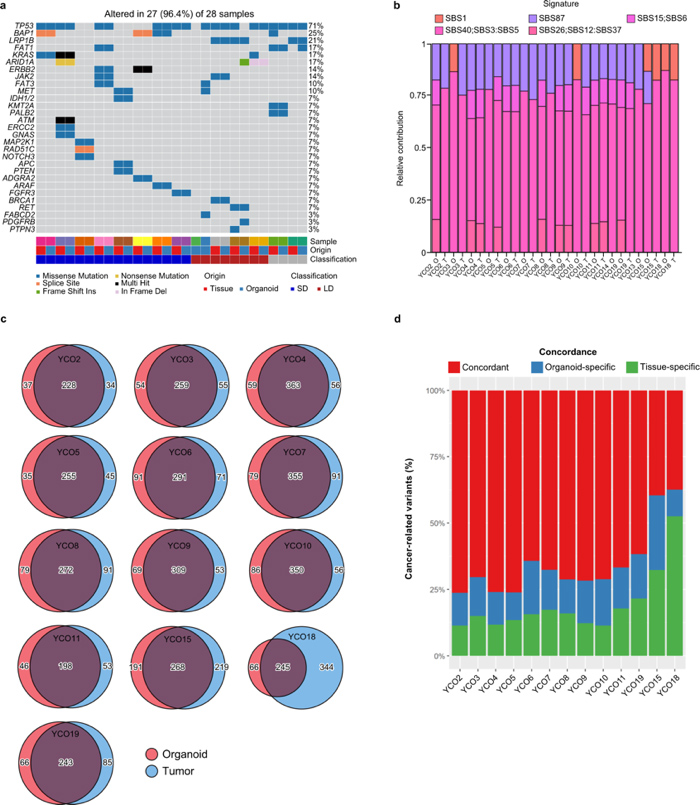
图3
3、根据转录组分析区分ICC亚型及功能富集分析和蛋白质互作网络(PPI)构建
根据ICC类器官的导管类型,利用RNA测序研究其转录组学特征,结果显示SD型和LD型ICC类器官的mRNA表达水平存在显著差异。其中,GPRC5A、MUC5AC、和TFF1在LD型类器官中高表达,而APOE、SPARC和BMP10在SD型类器官中高表达。
基因集富集分析结果显示LD型ICC类器官比SD型表现出“胆管癌2类”、“KRAS依赖性”、“TGFβ-up基因”和“ERBB-up基因”特征的显着富集。PPI网络分析显示,与LD型ICC类器官相关的关键转录因子包括ATF2、ELK1、CTNNB1、FLI1和ZNF217。
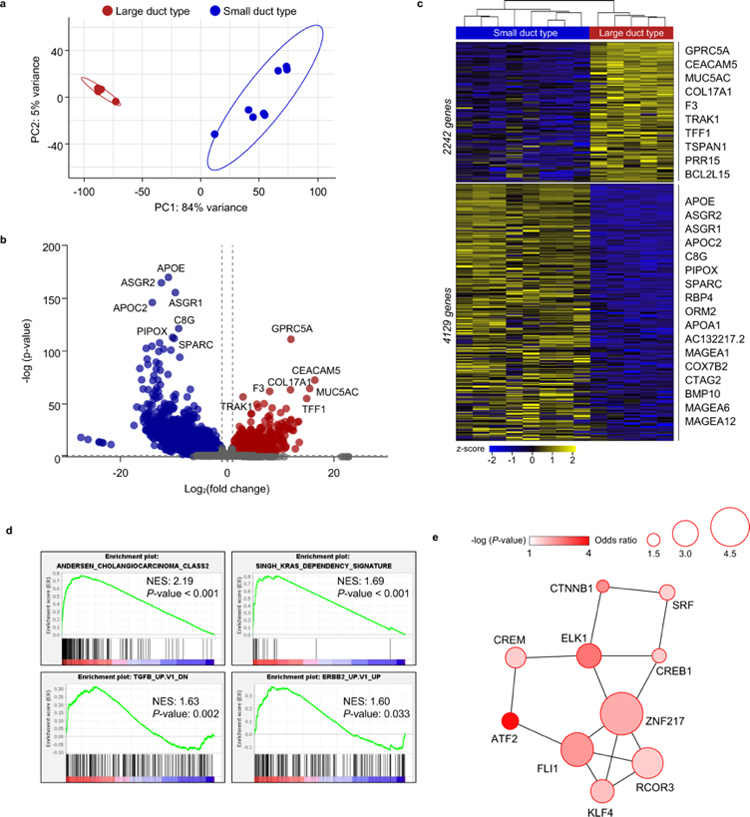
图4
4、ICC类器官预测患者的治疗效果
有研究表明SD型ICC比LD型预后更好[12, 13]。对患者临床数据和相应类器官的药物反应的分析结果显示,LD型中吉西他滨和顺铂组合的IC50高于SD型。然而,由于本研究的样本量较小,因此患者之间按亚型进行简单比较的价值有限。对患者临床数据和肿瘤特征的进一步研究表明,SD型患者的肿瘤中位数(6.9 cm)相比LD型患者(4.2 cm)更大,且无论其亚型如何,癌症分期都更晚。
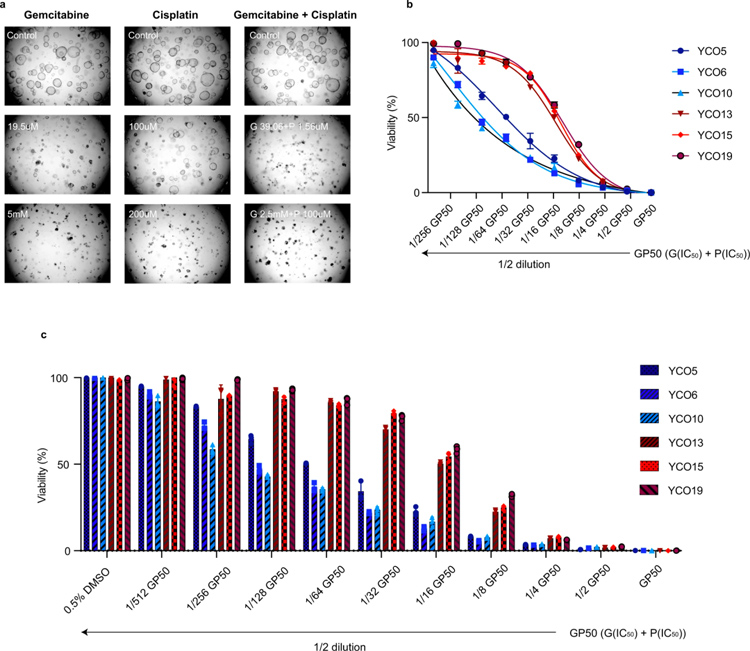
图5
二、编者点评:
本研究旨在开发一种个性化的、由患者衍生的、ICC亚型特异性模型。当前研究中开发的类器官模型可以克服组织质量的限制,模拟患者特征,深入研究对癌变和癌症的发展以及可靶向途径的发现,并为其他转化研究提供平台。
作为斑马鱼生物技术的全球领导者,环特生物搭建了“斑马鱼、类器官、哺乳动物、人体”四位一体的综合技术服务体系,开展科研及研发服务、智慧实验室建设和精准医疗三大业务。目前,环特类器官平台已成功搭建多种肿瘤类器官的培养平台,已有多种肿瘤类器官培养试剂盒和试剂在售,即将推出药物毒性检测服务,敬请期待!
参考资料:
[1]. Khan, S. A., Tavolari, S. & Brandi, G. Cholangiocarcinoma: epidemiology and risk factors. Liver Int. 39, 19–31 (2019).
[2]. Razumilava, N. & Gores, G. J. Cholangiocarcinoma. Lancet 383, 2168–2179 (2014).
[3]. Brindley, P. J. et al. Cholangiocarcinoma. Nat. Rev. Dis. Prim. 7, 65 (2021).
[4]. Bekaii-Saab, T. S., Bridgewater, J. & Normanno, N. Practical considerations in screening for genetic alterations in cholangiocarcinoma. Ann. Oncol. 32, 1111–1126 (2021).
[5]. Banales, J. M. et al. Cholangiocarcinoma 2020: the next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 17, 557–588 (2020).
[6]. Liau, J. Y. et al. Morphological subclassification of intrahepatic cholangiocarcinoma: etiological, clinicopathological, and molecular features. Mod. Pathol. 27, 1163–1173 (2014).
[7]. Kendall, T. et al. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 39, 7–18 (2019).
[8]. Hayashi, A. et al. Distinct clinicopathologic and genetic features of 2 histologic subtypes of intrahepatic cholangiocarcinoma. Am. J. Surg. Pathol. 40, 1021–1030 (2016).
[9]. Akita, M. et al. Histological and molecular characterization of intrahepatic bile duct cancers suggests an expanded definition of perihilar cholangiocarcinoma. HPB 21, 226–234 (2019).
[10]. Akita, M. et al. An immunostaining panel of C-reactive protein, N-cadherin, and S100 calcium binding protein P is useful for intrahepatic cholangiocarcinoma subtyping. Hum. Pathol. 109, 45–52 (2021).
[11]. Akita, M. et al. Dichotomy in intrahepatic cholangiocarcinomas based on histologic similarities to hilar cholangiocarcinomas. Mod. Pathol. 30, 986–997 (2017).
[12]. Chung, T. & Park, Y. N. Up-to-date pathologic classification and molecular characteristics of intrahepatic cholangiocarcinoma. Front. Med. 9, 857140 (2022).
[13]. Yoon, J. G. et al. Molecular characterization of biliary tract cancer predicts chemotherapy and programmed death 1/programmed death-ligand 1 blockade responses. Hepatology 74, 1914–1931 (2021).
[14]. Komuta, M. Intrahepatic cholangiocarcinoma: tumour heterogeneity and its clinical relevance. Clin. Mol. Hepatol. 28, 396–407 (2022).
[15]. Broutier, L. et al. Human primary liver cancer-derived organoid cultures for disease modeling and drug screening. Nat. Med. 23, 1424–1435 (2017).
[16]. Saito, Y. et al. Induction of differentiation of intrahepatic cholangiocarcinoma cells to functional hepatocytes using an organoid culture system. Sci. Rep. 8, 2821 (2018).
[17]. Wang, Z. et al. Conversion therapy of intrahepatic cholangiocarcinoma is associated with improved prognosis and verified by a case of patient-derived organoid. Cancers 13, 1179 (2021).
[18]. Li, L. et al. Human primary liver cancer organoids reveal intratumor and interpatient drug response heterogeneity. JCI Insight 4, e121490 (2019).
[19]. Maier, C. F. et al. Patient-derived organoids of cholangiocarcinoma. Int. J. Mol. Sci. 22, 8675 (2021).
[20]. Saito, Y. et al. Establishment of patient-derived organoids and drug screening for biliary tract carcinoma. Cell Rep. 27, 1265–1276.e1264 (2019).
